
Low Appetite in ME/CFS and Long COVID

When you live with a postviral condition like ME/CFS or long COVID, you expect fatigue, pain, or brain fog. But what about losing your appetite?
For some, hunger cues become weak, delayed, or almost absent. Eating feels like an afterthought until weakness, shakiness, dizziness, or extra fatigue shows up. Sometimes those symptoms are the only sign that the body is running low on fuel. ME/CFS and long COVID are complex conditions. But when intake drops too low for too long, undernourishment can add another layer of stress to an already stressed system.
A 2024 exploratory study found that after COVID-19, some people had changes in appetite-related hormones and brain activity in regions involved in appetite regulation, suggesting that hunger signaling may remain altered after infection (Inceu, 2024). In ME/CFS, earlier research found that dietary intake and lifestyle factors were associated with fatigue and functional impairment, which supports paying attention to basic nourishment even when appetite is low (Goedendorp, 2009).
This post explains why appetite can change in postviral illness, how to recognize possible signs of undereating, and practical ways to meet your needs when hunger cues are not reliable.
A note on fasting and caloric restriction:
I’m well known for discussing the benefits of therapeutic fasting and caloric restriction. Those strategies can have value in specific contexts, but they are very different from unintentionally eating too little because illness has blunted your appetite. Appetite loss in ME/CFS and other post-viral conditions is unintentional, often prolonged, and can quickly lead to undernourishment if not addressed. Recognizing the difference is crucial—this post is about meeting your body’s needs when hunger cues fail.
Why Appetite Changes Happen in Postviral Conditions
Many think of appetite as a simple signal: you get hungry, you eat, and your body feels satisfied. But hunger is regulated by the brain, gut, immune system, hormones, nervous system, and sensory cues. In ME/CFS and long COVID, several of those systems may be disrupted at the same time.
Low appetite may come from several overlapping factors.
1. Immune signaling
Loss of appetite during illness is part of a biological response often called “sickness behavior.” During infection or inflammation, immune signals can communicate with the brain and reduce appetite, food-seeking behavior, and motivation to eat (Gautron, 2010).
This can be useful during a short-term infection. But in postviral illness, some seem to remain stuck in a state where the body still behaves as if it needs to conserve energy, rest, and deprioritize digestion. It means the immune system and brain are communicating in ways that can change hunger.

2. Appetite hormones and brain signaling
Appetite is also shaped by hormones such as ghrelin and neuropeptide Y, which help regulate hunger and food intake.
In an exploratory study of adults after COVID-19, researchers found higher levels of appetite-related hormones and correlations with brain activity in regions involved in appetite regulation. Interestingly, self-reported hunger and desire to eat were not significantly different between groups (Inceu, 2024).
The study does not prove that long COVID always causes low appetite. But it does support the broader point that appetite regulation after COVID may be altered in ways that are not always obvious.
3. Smell and taste changes
After COVID specifically, appetite loss is tied to smell and taste changes. Food may smell strange, taste flat, taste metallic, or feel unpleasant. When food no longer smells or tastes normal, eating can feel like a task instead of a source of relief.
A 2026 study on persistent COVID-related smell and taste dysfunction found that these changes can affect appetite, hunger, food enjoyment, and quality of life (van Dijk, 2026).
4. Gut and autonomic symptoms
Low appetite can also come from digestive and autonomic symptoms. Nausea, reflux, bloating, IBS, slower motility, gastroparesis-like symptoms, and constipation can all make eating harder.
For people with orthostatic intolerance or POTS-like symptoms, eating upright may also worsen symptoms. Some people feel more lightheaded, flushed, tired, or uncomfortable after meals because digestion shifts blood flow toward the gut.
In those cases, the problem is not simply “lack of hunger.” Eating itself may feel physically demanding.
5. Low energy and sensory load
Even when food is available, the steps around eating can be too much.
Planning meals, shopping, cooking, smelling food, chewing, swallowing, washing dishes, and deciding what to eat all require energy. For someone with postviral illness, that load can be enough to delay or skip meals.
This is one reason appetite loss can become a cycle. The less you eat, the weaker you may feel. The weaker you feel, the harder it becomes to prepare food.
Signs You May Not Be Eating Enough
When hunger cues are unreliable, it is easy to undereat without realizing it. For many with ME/CFS or long COVID, the first clue is not a growling stomach. It is feeling weaker, shakier, colder, or more exhausted than usual.
Possible signs of undereating include:
feeling shaky, weak, or lightheaded between meals
sudden drops in energy after minor activity
worsening fatigue that improves somewhat after eating
feeling unusually cold
headaches, irritability, or anxiety-like symptoms when meals are delayed
weight loss or looser clothing
loss of muscle or strength
slower recovery after activity
waking at night feeling wired, hungry, or unsettled
constipation from low food volume, low fluid intake, or low overall intake
These symptoms can have many causes. They do not automatically mean you are undereating. But if they appear alongside low appetite, skipped meals, weight loss, or very low intake, food intake is worth looking at.
Why Calories Still Matter When Activity Is Low
A common assumption is that if you are resting most of the day, you do not need much food. Lower activity can indeed reduce calorie needs. But the body still needs energy for basic functions: brain activity, circulation, breathing, immune surveillance, digestion, tissue repair, temperature regulation, and maintaining muscle.
Even with reduced activity, eating too little can make symptoms worse. It can contribute to weakness, blood sugar swings, loss of lean mass, poor recovery, and lower resilience during infections or flares.
This is especially important for people who are newly ill, losing weight, mostly bedbound, or struggling to maintain basic intake.
How Many Calories Do You Need When Appetite Is Low?
There is no gold-standard calorie formula for ME/CFS or long COVID. Needs vary based on body size, illness severity, body composition, activity level, weight changes, inflammation, age, medications, and other medical conditions.
As a rough clinical reference, nutrition guidelines for medically vulnerable or older adults often use about 25–30 kcal per kg of body weight per day as a starting point, adjusted to the individual (Volkert, 2022). This is not an ME/CFS-specific rule, but it can help show how easy it is to fall short when appetite is very low.
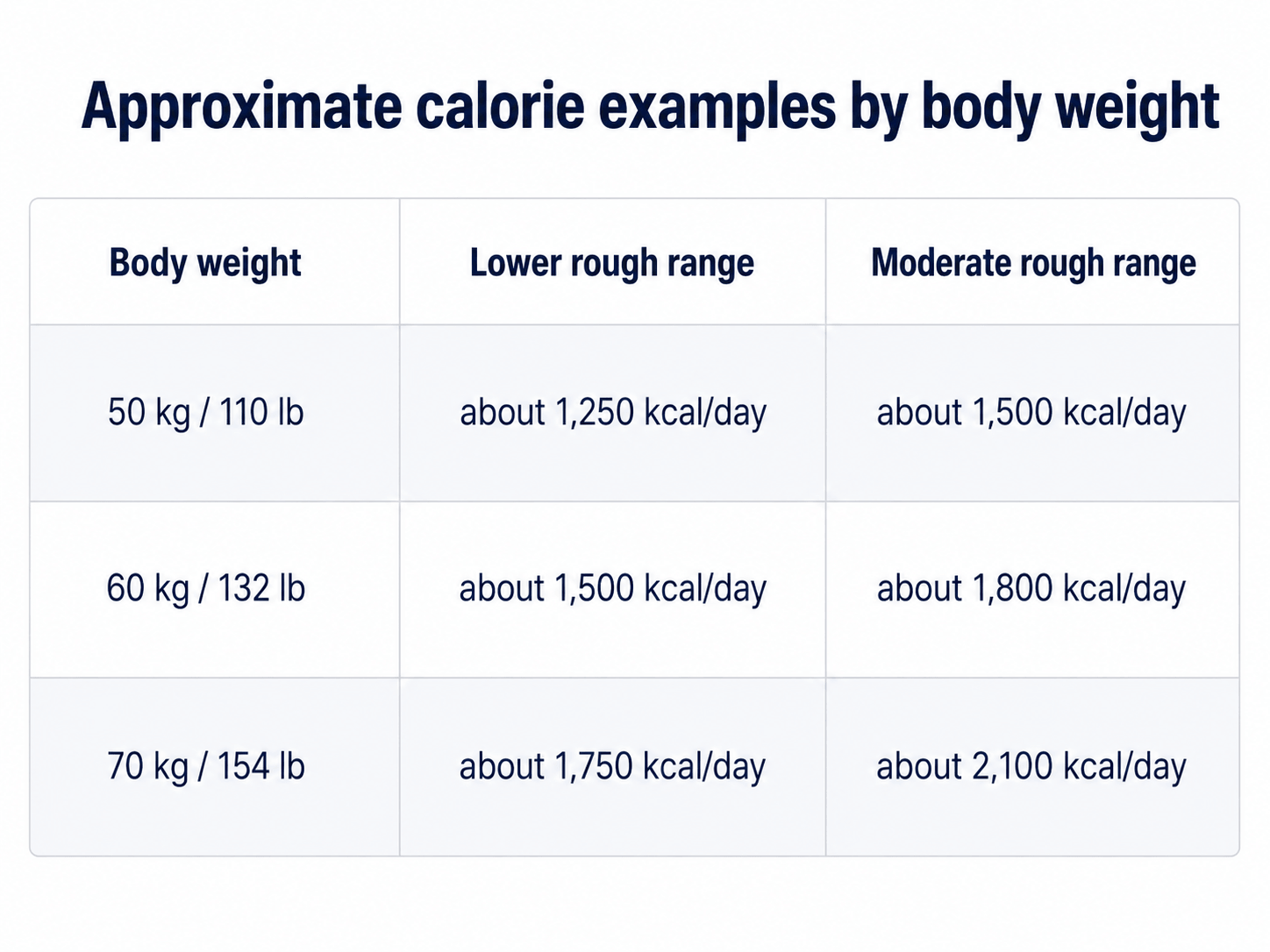
These are benchmarks, not hard-and-fast limits. Some people may need less. Others may need more, especially with weight loss, muscle loss, menstruation, healing needs, or higher activity.
The main point is this: if you are only managing a few bites here and there, a coffee/tea, a small snack, and half a dinner, you may be eating far less than your body needs.
Do Not Forget Protein
Protein helps maintain muscle, support immune function, and repair tissues. This becomes especially important when activity is reduced, because muscle can decline quickly with prolonged rest. Read more about protein needs in another post.
Expert recommendations for older adults often suggest at least 1.2 g of protein per kg of body weight per day, with higher needs in some people with acute or chronic illness (Deutz, 2014). These numbers are not specific to ME/CFS or long COVID (and I generally recommend a bit more), but they are useful as a general reminder: low intake can quickly become low protein intake too.
Protein intake is easier than you think. Eggs, Greek yogurt, cottage cheese, fish, chicken, tofu, protein powders, collagen added to other protein sources, lentils, and beans, depending on individual tolerance.
Easy Ways to Eat More Without Large Meals

When appetite is low, the goal is not to force large meals. The goal is to make eating easier, smaller, and more calorie-dense.
A few strategies can help:
Eat by schedule instead of waiting for hunger cues.
Try smaller meals or snacks every 3–4 hours.
Add calorie-dense foods such as olive oil, avocado, nut butter, tahini, full-fat yogurt, or cheese.
Use smoothies or shakes when chewing or cooking feels exhausting.
Keep no-prep foods available, such as Greek yogurt, eggs, hummus, canned fish, soup, protein shakes, cottage cheese, or ready-made meals.
Prioritize protein when intake is low.
Repeat simple meals instead of trying to create variety every day.
Eat semi-reclined or rest after meals if upright eating worsens symptoms.
The best option is the one you can actually manage during a flare.
When Low Appetite Needs Medical Attention
Low appetite is common during illness, but it should not be ignored if intake is very low or weight is dropping.
Seek medical support if you have unintentional weight loss, dehydration, persistent vomiting or diarrhea, severe abdominal pain, trouble swallowing, fainting, or very low intake for more than a few days.
Also, get guidance if you have coexisting medical conditions, a history of an eating disorder, or prolonged under-eating. In some cases, increasing food intake too quickly after a very low intake needs medical supervision.
The Bottom Line
Low appetite in ME/CFS and long COVID is not always just a digestive issue. It may involve immune signaling, appetite hormones, brain regulation, smell and taste changes, autonomic symptoms, medications, and the effort required to prepare food.
But even when hunger cues fail, the body still needs nourishment.
If you are weak, shaky, dizzy, losing weight, colder than usual, or crashing harder after small amounts of activity, it may be worth asking whether you are eating enough to support your basic needs.
This does not mean forcing large meals. It means using practical strategies: smaller portions, calorie-dense foods, protein, smoothies, no-prep options, and a simple eating rhythm that does not depend entirely on hunger. In postviral illness, food does not have to be perfect. But getting enough can matter.
FAQ: Frequently Asked Questions About Low Appetite in ME/CFS and Long COVID
-
Low appetite can happen in ME/CFS and long COVID, although not everyone experiences it. Some people feel less hungry because of nausea, smell and taste changes, autonomic symptoms, medication side effects, or immune-related changes in appetite signaling.
-
Hunger cues can become unreliable during illness. In postviral conditions, the immune system, nervous system, gut, brain, and appetite hormones may all influence hunger. This means you may feel weak, shaky, dizzy, or more fatigued before you actually feel hungry.
-
Yes. Long COVID can affect appetite in several ways. Some people have ongoing smell or taste changes, nausea, digestive symptoms, or altered hunger cues after infection. These changes can make food less appealing, even when the body still needs nourishment.
-
ME/CFS may affect hunger cues indirectly through fatigue, autonomic dysfunction, digestive symptoms, sensory sensitivity, and the energy required to prepare and eat food. Some people with ME/CFS do not feel strong hunger signals, especially during flares.
-
Possible signs include feeling shaky, weak, lightheaded, unusually cold, more fatigued between meals, or slower to recover after activity. Weight loss, looser clothing, loss of strength, and worsening symptoms when meals are delayed may also suggest that intake is too low.
-
There is no specific calorie formula for ME/CFS or long COVID. Needs vary by body size, activity level, illness severity, weight changes, and medical history. As a rough reference, many clinical nutrition guidelines use about 25–30 kcal per kg of body weight per day for medically vulnerable or low-activity adults, adjusted individually.
-
If your appetite is low but you are feeling weak, shaky, losing weight, or eating very little, it may help to eat by schedule instead of waiting for hunger. This does not mean forcing large meals. Small, calorie-dense meals or snacks are often more realistic.
-
Easy options include smoothies, protein shakes, Greek yogurt, eggs, soup, nut butter, avocado, hummus, cottage cheese, canned fish, soft grains, and ready-made meals. Adding olive oil, tahini, full-fat yogurt, cheese, or nut butter can increase calories without adding much volume.
-
No. Digestive symptoms can reduce appetite, but low appetite may also come from immune signaling, brain regulation, smell and taste changes, autonomic dysfunction, medications, or the effort required to prepare and eat food.
-
Seek medical support if you have unintentional weight loss, dehydration, persistent vomiting or diarrhea, severe abdominal pain, trouble swallowing, fainting, or very low intake for more than a few days. Also get guidance if you have coexisting health conditions, a history of an eating disorder, or prolonged under-eating.
References
Inceu G, Nechifor RE, Rusu A, et al. Post-COVID-19 Changes in Appetite-An Exploratory Study. Nutrients. 2024;16(14):2349. Published 2024 Jul 20. doi:10.3390/nu16142349
van Dijk B, Postma EM, Boek WM, Kamalski DMA, Boesveldt S. The impact of persistent COVID-19-related chemosensory dysfunction on quality of life, appetite and hunger: The COVORTS study. Appetite. 2026;218:108391. doi:10.1016/j.appet.2025.108391
Goedendorp MM, Knoop H, Schippers GM, Bleijenberg G. The lifestyle of patients with chronic fatigue syndrome and the effect on fatigue and functional impairments. J Hum Nutr Diet. 2009;22(3):226-231. doi:10.1111/j.1365-277X.2008.00933.x
Gautron L, Layé S. Neurobiology of inflammation-associated anorexia. Front Neurosci. 2010;3:59. doi:10.3389/neuro.23.003.2009
Volkert D, Beck AM, Cederholm T, et al. ESPEN practical guideline: Clinical nutrition and hydration in geriatrics. Clin Nutr. 2022;41(4):958-989. doi:10.1016/j.clnu.2022.01.024
Deutz NEP, Bauer JM, Barazzoni R, et al. Protein intake and exercise for optimal muscle function with aging: recommendations from the ESPEN Expert Group. Clin Nutr. 2014;33(6):929-936. doi:10.1016/j.clnu.2014.04.007